

Introduction
Venous thromboembolism (VTE) (deep vein thrombosis [DVT] and pulmonary embolism [PE]) is a cause of significant morbidity and mortality. Over the last decade, there has been an increase in awareness and major advances in early diagnosis and treatment of VTE. This study sought to estimate the mortality and associated diagnoses in hospitalized patients with a primary diagnosis of DVT or PE using a nationally representative database.
Methods
The 2017 Healthcare Cost and Utilization Project's Nationwide Inpatient Sample (HCUP-NIS) was used for analysis. The NIS uses a stratified probability sample of 20% of all inpatient discharges, representing over 97% of the US population. Sampling weights were applied to hospital discharges for DVT and PE using applicable ICD‐10 codes to generate nationally representative estimates. Pearson's chi-squared test and the Mann-Whitney U test were used for comparisons to assess statistical significance.
Results
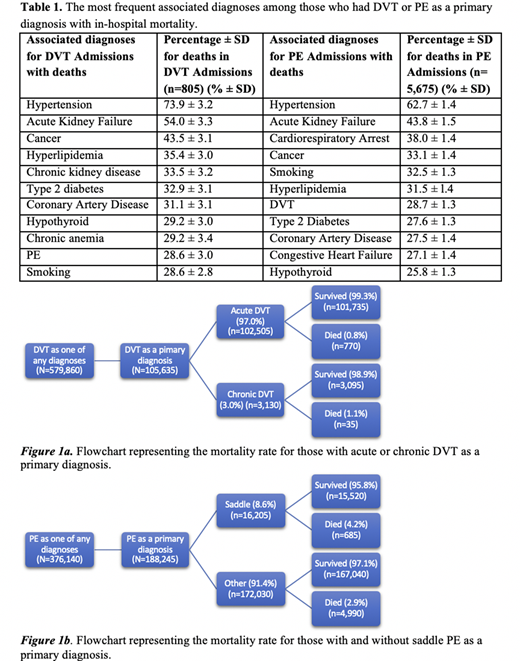
Of the nearly 36 million hospital admissions in 2017, 579,860 had DVT included in the index list of diagnoses during the hospitalization, and 105,635 had DVT as the primary admission diagnosis. Within the primary DVT admissions (median age (interquartile range (IQR)): 64 years (51-77)), 102,505 were acute DVT, and 3,130 were chronic DVT. There were 376,140 admissions with PE as one of all diagnoses and 188,245 with PE as the primary admission diagnosis. Among primary PE admissions (median age (IQR): 64 years (52-75)), 16,205 (8.6%) were saddle PE (Figure 1a). Overall, there were 826,155 people diagnosed with PE or DVT as one of any diagnoses, and 129,845 were diagnosed with both DVT and PE.
Mortality
The all-cause mortality in admissions with a primary diagnosis of DVT (0.8%) was significantly lower than for all other NIS admissions at 1.96% (p<0.001) (Figure 1a). Among primary DVT admissions who had in-hospital mortality, the median age (IQR) at death was 72 years (61-82), which was comparable to 73 years (61-83) for all other NIS hospitalizations. The median (IQR) length of stay (LOS) of primary DVT admissions who had in-hospital mortality was 5 days (3-10).
For primary PE admissions, the all-cause mortality (3.0%) was significantly higher than all other NIS admissions (p<0.001). Among the PE admissions, mortality in those with saddle PE (4.2%) was significantly higher than all other PE cases (p<0.001) (Figure 1b). The median (IQR) age at death for PE patients was 71 years (60-81) and was comparable to all other NIS hospitalizations. The median (IQR) LOS for deaths in PE admissions was 3 days (1-7).
Besides the known cardiovascular disease risk factors such as hypertension, obesity, smoking, Type 2 diabetes mellitus, and hyperlipidemia, the most common diagnoses in those who died with DVT or PE as a primary diagnosis were acute kidney failure, cancer, and chronic kidney disease (CKD) (Table 1).
Health Care Utilization
The median (IQR) hospital charges for DVT and PE admissions were $27,476 ($15,053-$54,874) and $29,158 ($17,471-$52,636) respectively. These were comparable to all NIS hospitalizations at $26,841 ($12,969-$54,568).
For hospitalizations for DVT and PE resulting in death, the median (IQR) hospital charges were $60,689 ($24,775-$137,830), and $55,218.50 ($29,373-$106,313) respectively which were comparable to all NIS deaths at $56,107 ($23,117-$131,768).
Discussion/Conclusions
In the United States, DVT or PE was listed as one of the discharge diagnoses in approximately 825,000 admissions in 2017 and was the primary reason for admission in 300,000 cases (0.8% of all admissions). PE was seen more often as a primary cause for hospitalization, while DVT was more often seen as a comorbidity.
The all-cause mortality among admissions for PE was greater than that for DVT. The subset of PE patients with saddle embolism had the highest mortality rate of all admissions for VTE.
Besides cardiovascular risk factors, cancer, acute kidney failure, and CKD were among the most common comorbidities seen in admissions with PE and DVT that had in-hospital mortality.
Streiff:Bayer: Consultancy, Speakers Bureau; Portola: Consultancy; Boehringer-Ingelheim: Research Funding; NHLBI: Research Funding; PCORI: Research Funding; NovoNordisk: Research Funding; Sanofi: Research Funding; Dispersol: Consultancy; BristolMyersSquibb: Consultancy; Janssen: Consultancy, Research Funding; Pfizer: Consultancy, Speakers Bureau. Takemoto:Novartis: Other: DSMB Aplastic Anemia Trial; Genentech: Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal